
Executive Summary
Limb tourniquets for field hemorrhage control are predominantly windlass devices such as the Combat Application Tourniquet (CAT) and ratcheting devices such as the Ratcheting Medical Tourniquet (RMT) (Altamirano et al., 2015; Efficacy of publicly accessible tourniquets, 2025). Windlass tourniquets use a rotating rod to tension a strap whereas ratcheting tourniquets use a mechanical buckle that advances the strap in discrete increments (Altamirano et al., 2015; Wall & Samutsakorn, 2019). Both architectures can achieve arterial occlusion when applied correctly yet they differ in the number and type of application steps and in how they maintain pressure over time, which affects mechanical reliability and usability in high stress settings (Altamirano et al., 2015; Kragh et al., 2013; Wall & Samutsakorn, 2019).
Everyday users such as armed civilians and on/off duty officers operate under conditions that often include limited recent medical training and significant physiological stress. In these circumstances fine motor control is reduced and body position may be constrained. Designs that require multiple precise steps including complex strap routing and manual rod securing may be more vulnerable to error than designs that rely on a smaller set of gross motor actions with built in locking at each increment of tightening (Efficacy of publicly accessible tourniquets, 2025; Tourniquet self-application assessment in cold weather conditions, 2023; Wall & Samutsakorn, 2019). Data from military retrieval studies, experimental laboratory work, and layperson simulation studies collectively indicate that simplified application sequences and stable pressure maintenance under movement are associated with higher practical performance and lower misapplication rates (Altamirano et al., 2015; Efficacy of publicly accessible tourniquets, 2025; Kragh et al., 2013; Wall & Buising, 2026).
Everyday carry context
For everyday carry a limb tourniquet must satisfy several practical conditions. The device must be small and flat enough to integrate into typical carry methods such as pockets, ankle kits, or belt mounted pouches. It must be realistically self applied to upper and lower extremities with one hand or with limited use of the other hand. It must retain sufficient mechanical security to maintain arterial occlusion while the user changes position, moves to cover, or performs other tasks (Efficacy of publicly accessible tourniquets, 2025; Tourniquet self-application assessment in cold weather conditions, 2023). Many nonmedical carriers do not receive frequent refresher training. Survey and registry data suggest that tourniquet techniques can degrade over time without practice and misapplication rates remain substantial in both military and civilian populations (Kragh et al., 2013; Tourniquet-related complications in extremity injuries, 2025).
Within this context the choice between windlass and ratcheting designs is partly a question of user familiarity and partly a question of how many discrete steps the device demands from a person who may be under marked sympathetic activation. Evidence indicates that devices with mechanical advantage systems are generally more effective than improvised devices when used by laypeople, yet within that group some designs require less intensive training to achieve comparable performance (Efficacy of publicly accessible tourniquets, 2025).
Windlass tourniquet mechanics and performance
Windlass tourniquets use a strap, a buckle, and a cylindrical rod. In the CAT the strap passes through a friction buckle, slack is removed by manual pulling, and the windlass rod is rotated to shorten the strap and raise circumferential pressure until arterial flow is occluded (Kragh et al., 2013). The rod is then secured in a retaining device. Large military series confirm that properly applied CAT tourniquets can control life threatening limb hemorrhage and contribute to improved survival in both prehospital and combat settings (Kragh et al., 2013; Tourniquet-related complications in extremity injuries, 2025).
The entire PowerPoint presentation can be found here in PDF format: https://www.c-tecc.org/images/Underrecognized_Recurring_Tourniquet_Problems_April_2026.pdf
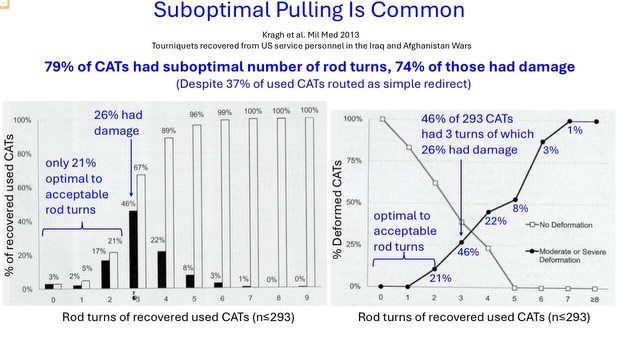
Field and experimental data also describe several limitations relevant to everyday carriers. Application to the thigh using one hand requires the user to generate rotational torque against a resistant limb, which can be difficult for individuals with reduced strength or unstable body positions (Altamirano et al., 2015; Tourniquet self-application assessment in cold weather conditions, 2023). Analyses of recovered CATs from combat casualties found that seventy nine percent had a suboptimal number of windlass turns and that seventy four percent of those displayed rod deformation or other damage, suggesting repeated attempts to compensate for inadequate strap pre tension (Kragh et al., 2013). Only about twenty one percent of devices fell within an optimal or acceptable rod turn range (Kragh et al., 2013).
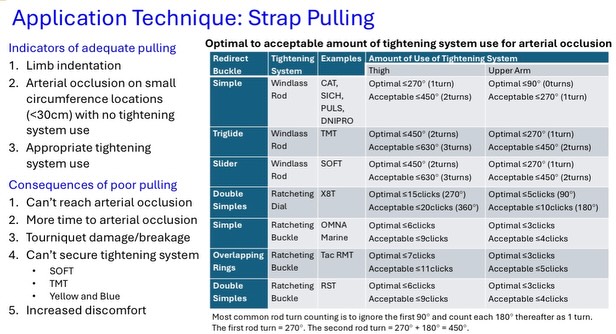
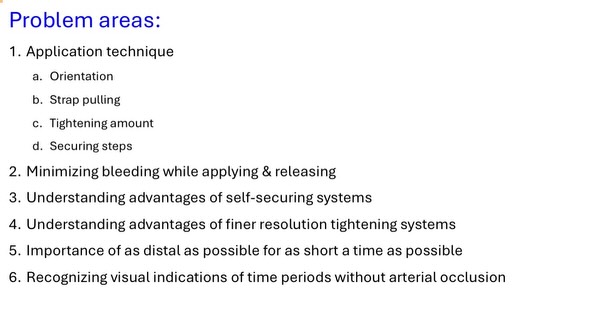
Work by Wall and colleagues indicates that strap pulling technique strongly influences secured strap pressure. Pulling tangentially around the limb near the buckle yields higher initial compression than pulling upward from a distant point on the strap (Wall & Samutsakorn, 2019). The Committee on Tactical Combat Casualty Care (CoTCCC) Tourniquet Working Group notes that application technique, strap pulling, tightening amount, and securing steps are recurrent problem areas in both training and operational use (Wall & Buising, 2026). Slides from that group indicate that inadequate pulling is associated with prolonged time to occlusion, incomplete occlusion, increased device damage, and increased discomfort (Wall & Buising, 2026).
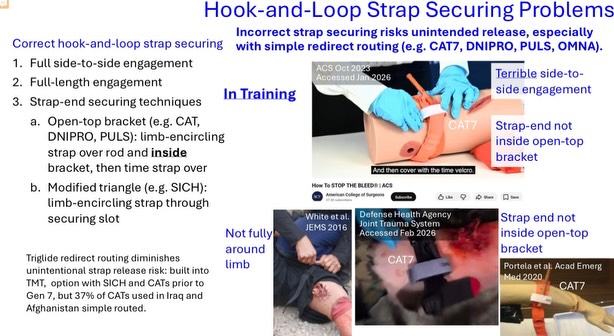
“Incorrect strap securing risks unintended release, especially with simple redirect routing” -Wall, P. L., & Buising, C. (2026, April 27). Underrecognized, Recurring Tourniquet Problems [Conference presentation]. Committee on Tactical Combat Casualty Care Meeting, slide “Hook-and-Loop Strap Securing Problems.”
Windlass systems also rely on specific hook and loop routing patterns for mechanical stability. The CoTCCC presentation on “Hook and Loop Strap Securing Problems” documents errors in which the strap is not fully wrapped around the limb, not routed inside the open top bracket, or engaged only partially across its width (Wall & Buising, 2026). Such configurations increase the risk of unintentional release or gradual loosening during movement. Even with design revisions, a substantial fraction of CATs in military series were routed using simple redirects that bypass stabilizing features designed to reduce release risk (Kragh et al., 2013; Wall & Buising, 2026).
Overall these findings suggest that windlass designs function effectively when users apply strong pre tension, follow recommended routing, and secure the rod correctly. They also indicate that deviations from these steps are common in field conditions, particularly when users are under stress or have limited recent training (Altamirano et al., 2015; Kragh et al., 2013; Tourniquet-related complications in extremity injuries, 2025).
Ratcheting tourniquet mechanics and performance
Ratcheting medical tourniquets replace the windlass rod with a ratcheting buckle. In the Ratcheting Medical Tourniquet (RMT) the user threads the strap into the buckle, pulls to tighten, and each pull advances the strap by one or more teeth while a pawl prevents reverse motion (Wall & Samutsakorn, 2019). The Committee on Tactical Combat Casualty Care lists the RMT Tactical model as a recommended limb tourniquet and describes it as a one handed device for limb hemorrhage control (CoTCCC Recommended Devices and Adjuncts, 2021).
Laboratory evaluations in human limb models have reported high rates of successful arterial occlusion with the RMT and relatively low rates of pressure loss over short observation periods when devices were applied according to manufacturer guidance (Wall & Samutsakorn, 2019). The incremental action of the ratchet provides discrete feedback through audible clicks and tactile resistance and allows users to increase pressure gradually until bleeding stops or distal pulses are absent (Wall & Samutsakorn, 2019). Because the ratchet locks at each increment, movement or jostling alone does not reverse strap advancement and mechanical stability does not depend on seating a separate rod in a clip.
A systematic review of layperson tourniquet performance found that commercially manufactured tourniquets with mechanical advantage systems, including both windlass and ratcheting designs, enabled untrained or minimally trained individuals to achieve vascular occlusion on simulation models at high rates (Efficacy of publicly accessible tourniquets, 2025). The review noted that user friendly designs and brief structured instruction improved performance and suggested that devices requiring fewer precise steps may help mitigate misapplication among nonmedical responders (Efficacy of publicly accessible tourniquets, 2025).
Self application and environmental factors
Self application is a critical capability for everyday users. A field study conducted in cold weather among nonmedical civilians assessed self application of five commercial extremity tourniquets, including the CAT and the RMT, over winter clothing (Tourniquet self-application assessment in cold weather conditions, 2023). After a brief training module participants were able to self apply four of the five designs to upper and lower extremities using one handed and two handed techniques and achieve vascular occlusion, although ease of use ratings varied by device (Tourniquet self-application assessment in cold weather conditions, 2023). The ratcheting marine tourniquet tested in that study received high scores for application ease, indicating that this architecture can be used effectively under realistic environmental constraints with appropriate instruction (Tourniquet self-application assessment in cold weather conditions, 2023).
These results suggest that training level and environmental conditions interact with device design. When users receive structured instruction shortly before use, both windlass and ratcheting tourniquets can be self applied successfully even while wearing cold weather gloves (Tourniquet self-application assessment in cold weather conditions, 2023). In contrast, registry and scoping review data indicate that in broader practice settings where training is variable and time since last practice is longer, misapplication rates and complication risks increase (Efficacy of publicly accessible tourniquets, 2025; Tourniquet-related complications in extremity injuries, 2025).
Device variants and specific populations
The RMT family includes models with different strap widths and configurations, including 1.5 inch and 2 inch versions and pediatric oriented designs and high strength stainless steel variants (1.5 inch Ratcheting Medical Tourniquet, 2017; Ratcheting Medical Tourniquet, 2″, 2025). Wider straps distribute pressure over a larger area, which can reduce focal soft tissue loading and may improve comfort during prolonged application, while narrower low profile designs facilitate integration into slim everyday carry setups (Wall & Samutsakorn, 2019; Ratcheting Medical Tourniquet, 2″, 2025).

Pediatric trauma data show that limb tourniquet use by a mix of bystanders, first responders, and clinicians can be feasible and safe for children when appropriately indicated. A single center cohort of injured children reported no adverse events attributable to tourniquet use and a high proportion of properly applied devices across prehospital and hospital settings (Pediatric tourniquet use: Safe and effective, 2025). Purpose built pediatric ratcheting tourniquets aim to match smaller limb circumferences more closely than many adult windlass devices, although comparative outcome data for specific pediatric designs remain limited (Pediatric tourniquet use: Safe and effective, 2025).
Implications for everyday selection
Current evidence indicates that both windlass and ratcheting tourniquets can achieve effective hemorrhage control when applied correctly yet they differ in their sensitivity to specific application errors and in their integration with everyday carry constraints. Windlass designs such as the CAT have a large evidence base in military and tactical contexts and are widely taught in formal courses. Ratcheting designs such as the RMT have a smaller but growing evidence base and incorporate mechanical features intended to simplify application and maintain pressure with fewer discrete securing steps (CoTCCC Recommended Devices and Adjuncts, 2021; Efficacy of publicly accessible tourniquets, 2025; Wall & Samutsakorn, 2019).

For users who train regularly with a specific windlass device and operate in systems built around that device, maintaining that platform may maximize consistency. For users with infrequent medical training, variable grip strength, or strong constraints on carry profile, ratcheting designs offer characteristics that may improve practical usability and mechanical reliability. In all cases available studies emphasize that structured training and periodic practice are critical determinants of effective tourniquet use, regardless of device type (Efficacy of publicly accessible tourniquets, 2025; Tourniquet-related complications in extremity injuries, 2025; Wall & Buising, 2026).
Ratcheting tourniquet designs incorporate features specifically intended to reduce the training burden on everyday carriers and non-medical users who may not receive frequent refresher instruction. The RMT‘s self-securing ratcheting mechanism eliminates multiple precision-dependent steps that characterize windlass designs, including optimal strap pulling technique, correct windlass rod rotation, and proper hook-and-loop securing procedures (Wall & Buising, 2026). Each incremental advancement of the ratchet automatically locks in place through a pawl mechanism, providing both tactile and audible feedback through discrete clicks that guide users toward arterial occlusion without requiring them to master nuanced techniques such as tangential strap pulling or specific rod turn counts (Wall & Samutsakorn, 2019). Research by Portela and colleagues demonstrated that among laypersons applying tourniquets using only manufacturer instructions, the RMT achieved the highest effective application rate at 64.4 percent and was the most rapidly applied device, suggesting that its design successfully translates into intuitive use even among completely untrained individuals (Efficacy of publicly accessible tourniquets, 2025). This training-minimized architecture directly addresses the reality that many everyday carriers operate with limited recent medical training and face degraded fine motor control under physiological stress (Efficacy of publicly accessible tourniquets, 2025).
The RMT‘s design philosophy prioritizes gross motor actions and built-in mechanical safeguards over user-dependent technique, which experimental evidence suggests reduces misapplication vulnerability in high-stress scenarios. Wall and Buising’s 2026 analysis of tourniquet application processes across 512 applications found that tightening-system mechanical problems were substantially more frequent with windlass rod systems, including 26 instances of losing hold of the rod, 27 instances of redoing rod turns, and 58 instances of struggling to secure the rod, compared to only 3 tooth skips and 16 advance failures across all ratchet systems tested. Furthermore, 103 of 109 improperly secured applications involved non-self-securing design features of windlass devices, whereas ratcheting systems demonstrated fewer securing errors due to their self-locking architecture. The Committee on Tactical Combat Casualty Care’s designation of the RMT as a “one handed” device for limb hemorrhage control reflects recognition that its design accommodates users with compromised hand strength, limited mobility, or constrained body positions, conditions common in self-application scenarios where formal training protocols may not be recently rehearsed (CoTCCC Recommended Devices and Adjuncts, 2021). By engineering around common application errors rather than relying on user training to prevent them, ratcheting designs offer a mechanical solution to the training-time problem that affects civilian carriers, off-duty personnel, and other populations for whom frequent refresher courses may not be realistic (Tourniquet self-application assessment in cold weather conditions, 2023).
Multiple versions of the CoTCCC Recommended Ratcheting Medical Tourniquet, including the marine and pediatric versions can be purchased at VDEV.GROUP.
References
1.5 inch Ratcheting Medical Tourniquet (RMT) Tactical. (2017). V Development Group. https://vdev.group/products/1-5-ratcheting-medical-tourniquet-rmt-tactical
Altamirano, M. P., Wall, P. L., Kelly, J. P., Porterfield, J. R., & Kragh, J. F. (2015). Role of the windlass in improvised tourniquet use on a manikin hemorrhage model. Wilderness & Environmental Medicine, 26(4), 516–524. https://pubmed.ncbi.nlm.nih.gov/26125163
CoTCCC Recommended Devices and Adjuncts. (2021). Committee on Tactical Combat Casualty Care. https://learning-media.allogy.com/api/v1/pdf/ef9c8ec7-c4b2-4948-9ff5-fb34f504032a/contents
Efficacy of publicly accessible tourniquets: A systematic review of layperson performance utilizing simulation models. (2025). Advances in Simulation, 10, 57. https://pmc.ncbi.nlm.nih.gov/articles/PMC12625582
Kragh, J. F., O’Neill, M. L., Walters, T. J., Jones, J. A., Baer, D. G., Gershenbaum, M., & Wade, C. E. (2013). Analysis of recovered tourniquets from casualties of Operation Enduring Freedom and Operation New Dawn. Military Medicine, 178(7), 806–810. https://pubmed.ncbi.nlm.nih.gov/23820356
Pediatric tourniquet use: Safe and effective. (2025). Journal of Pediatric Surgery, 60(4), 555–562. https://pmc.ncbi.nlm.nih.gov/articles/PMC12412217
Ratcheting Medical Tourniquet (RMT), 2″. (2025). Rescue Essentials. https://rescue-essentials.com/m2-ratcheting-medical-tourniquet
Tourniquet-related complications in extremity injuries: A scoping review of the literature. (2025). Injury, 56(7), 1359–1374. https://pmc.ncbi.nlm.nih.gov/articles/PMC12188649
Tourniquet self-application assessment in cold weather conditions. (2023). Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 31, 82. https://pmc.ncbi.nlm.nih.gov/articles/PMC10472695
Wall, P. L., & Buising, C. (2026, April 27). Underrecognized recurring tourniquet problems [Conference presentation]. Committee on Tactical Combat Casualty Care Meeting. https://www.instagram.com/p/DXwk6wSFWZh
Wall, P. L., & Samutsakorn, R. (2019). Best tourniquet holding and strap pulling technique. Journal of Special Operations Medicine, 19(2), 36–44. https://jsomonline.org/wp-content/uploads/2024/02/2019248Wall.pdf





Leave a comment